
This article is based on the Mick Cooper’s “Essential Research Findings in Counselling and Psychotherapy, Facts are Friendly” book compiling studies of effectiveness in counselling and psychotherapy. It is a great reference book and I am leaving most data behind (so that you buy the book, which is fantastic).
What therapy is most effective for what?
Research in psychotherapy has attempted to provide an answer to this question. This journey has been made in squiggly, rather than straight lines.
Such is the degree of controversy in this topic than reading Mick’s excellent chapter on this topic will leave you a bit dizzy (but much wiser) as you go through the back and forth of the different research that has been piled on therapy effectiveness.
To start with, we can’t find out what therapy is the most effective if we can’t agree on what it is to be effective for. And this is where controversy starts.
What’s therapy for?
Proponents of the “differential effectiveness” are influenced by the Western bio-medical model and argue for distinctiveness and separatedness. According to people in this camp, some forms of therapy will be most effective for some issues (symptoms or mental disorders) and therefore the trick is to optimise which therapy is best for each symptom.
Through this lens, it is Cognitive and Behavioural orientations the ones that have the most evidence to prove its effectiveness. We will put this in the microscope too, but let’s stay in the differential effectiveness view for now.
There are therapists who argue against this position in principle. They will point out that isolated disorders hardly exist (over 40% of those who meet criteria for a diagnosis will meet criteria for at least a second diagnosis, see research). They will also argue and that therapy is not necessarily to “treat anxiety” or any other specific condition, offering instead a more holistic, fundamental vision of mental wellbeing.
This philosophical disagreement in how the question is asked is a major barrier to effective collaboration in psychotherapy research.
Consider that Cognitive-behaviouralists are concerned with evidence-based decision-making and in using the scientific method to isolate processes and slowly increase our knowledge on how they work.
Because of this, they are natural adherents to using research and measurable outcomes (such as Beck inventory for depression) and are both motivated and successful at getting funding to do studies that attempt to isolate patients of a certain condition and prove how effective the therapies may be at treating such condition.
Once you add the effect of researcher allegiance (e.g cognitive therapists seek funding to prove that cognitive therapy works and therefore carry bias that compromise research design), you can see why it is that the Cognitive-behavioural school has the most evidence in treating depression, anxiety and other major mental health symptoms.
On the other hand, humanistic therapists are not as motivated to get funding for research because they are against the differential effectiveness perspective and because they have a more holistic understanding of what therapy is for.
The philosophical disagreement for and against the differential effectiveness perspective is a major barrier to effective collaboration in psychotherapy research.
They may feel less comfortable about how the research design may set parameters for what can happen in a session, or how many sessions will there be in total.
The cognitive-behavioural orientation has the most evidence for it because its the most suited for research and therefore where more research happens. More research, more evidence.
Not a satisfactory finding, if one has an agnostic mindset and likes to think deeply about things. So, let’s keep going.
If they exist, they must work
There is a neat little idea that tries to reconcile this complex debate: the dodo bird.
Mick’s Facts are Friendly discusses meta-analysis research and how studies that compare effectiveness vs control therapies show only a small difference between the type of therapy used by the therapist.
In short, there are no many studies where the effect of one type of therapy is much bigger than the effect of the other one: it seems not too matter that much.
The mental model of the dodo bird is that if a therapeutic approach is in practice today, it’s because it has shown effectiveness for enough people, for long enough to still being practiced and studied. Therefore, it has to work to some extent.
Of course, not everyone agrees with meta-analysis as being meaningful ways to compare studies. Some people will also add that the dodo bird is a weak argument against the hard (yet philosophically fragile) evidence.
But we need to move on, or we will never get to an answer.
Beyond the dodo bird: integrative therapy and pluralism
I believe that knowledge and perspective integration is a widespread trend in all domains of human endeavour. In our increasingly interconnected world the exchange of ideas is not only easier but often necessary for innovation.
Entire new fields are being born from integrating thinking from different perspectives (neuroscience, biotechnology, artificial intelligence) and old fields are rejuvenated by constantly adopting ideas from each other (design, fashion, business, media, manufacturing, technology).
In the same way, there should be little question that psychodynamic understanding of the unconscious can be integrated with the powerful moments of connection that person-centred therapists seek to provide and with useful and practical learnings from cognitive-behavioural therapies.
Mick himself was amongst the founders of pluralism, a philosophical stance that accepts the possible value that other therapies can bring when combined with the core conditions.
He has also done work to help therapists codify and integrate preferences of the client, a practice that executes Roger’s ultimate vision of empowerment.
In this video, Mick discusses pluralism:
How clients benefit from pluralist thought and integrative practice
The number and complexity of therapeutic orientations in the counselling and psychotherapy becomes a minefield for clients. I’m currently conducting an informal research project on the market.
One of the key findings in this study is that “Integrative” is the most popular “orientation” offered by therapists. Similarly, we have found big segments of therapists combining orientations from divergent schools of thought.
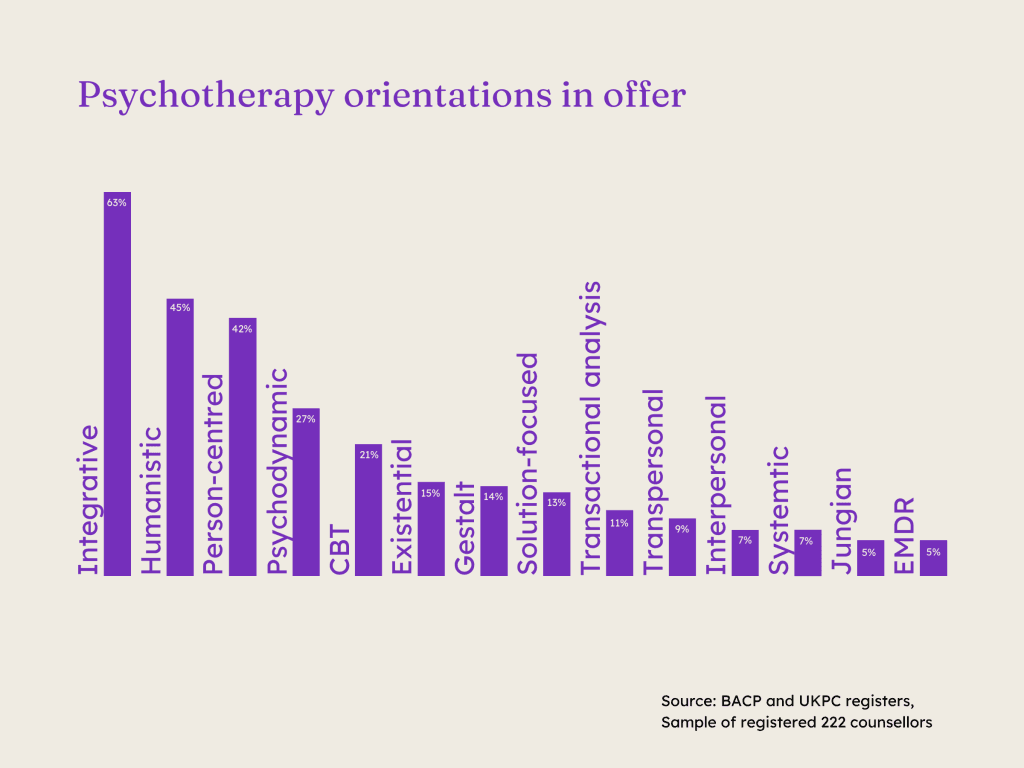
In short, psychotherapy is integrating.
We can’t possibly ask clients to engage as deeply as the industry does with the nuance of different orientations and the way they can work together. That’s not how markets tend to work in the long run – instead, they become user-centred.
Can you imagine being referred by a GP to a gastroenterologist, only to be told there are dozens of gastroenterological orientations with rich debates about their meaning and emphasis?
The expectation is that the specialist simplifies the information and provides a clear path forward. Similarly, in therapy, it wouldn’t be practical for clients to engage with complex debates between orientations—it’s up to the therapist to integrate, simplify and adapt these for the client’s benefit.
And it seems today’s therapists are embracing this too!
Research
What types of therapy are there in offer
I’m collaborating with Psychotherapeutic author Mick Cooper to explore the different types of psychotherapy available in the UK. Our goal is to understand how popular each type is and to develop a clear classification system that makes it easier for clients to navigate the therapy landscape.





